The way a baby attaches to the breast (latches) is important. If a baby has only got the nipple in his mouth, without a good mouthful of breast tissue, it will usually feel uncomfortable for the mother, and the baby is likely to struggle to get a full supply of milk. This is often called a “shallow latch”. Conversely, when baby has a big mouthful of the breast as well as the nipple, it means the mother’s nipple is deeper in the baby’s mouth where it will not get rubbed against the roof of baby’s mouth or by his tongue. With plenty of breast tissue as well as the nipple in a baby’s mouth (a deep latch), breastfeeding is comfortable, nipples are not sore, and the milk-making tissue in the breast can be stimulated to make a full milk supply.
This article
This article shares some tips for helping a baby to attach deeply and comfortably to the breast. For ways to position your baby before the latch see Breastfeeding Positions for Newborns or try watching some of these Breastfeeding Videos.
Top tips
Find a breastfeeding specialist
If possible, a great way to get help with positioning and attaching your baby to the breast is to see a breastfeeding specialist such as an IBCLC lactation consultant. An IBCLC will be able to suggest different positions and techniques based on yours and your baby’s anatomy. They can help with general breastfeeding tips before your baby is born so that you know what to expect or, if your baby has already arrived, they can help you avoid sore nipples or painful feeds.
Skin-to-skin contact
Skin-to-skin contact involves holding your baby without clothes or blankets coming between you. It is not essential for success, but one of the many benefits of skin-to-skin is that it can help a newborn baby use his natural instincts and feeding reflexes to help him latch deeply on his own. Holding your baby in skin-to-skin contact for a whole sleep cycle, not just for feeding, can be helpful too. See Why Skin-to-Skin? for further information on the benefits of skin-to-skin.


If it ain’t broke don’t fix it
The way a baby is attached to your nipple is often described as either a shallow latch or a deep latch.
- Shallow latch: when a baby has the nipple and only a shallow, small or superficial amount of breast tissue in their mouth. This is more likely to be painful and lead to low milk supply.
- Deep latch: when a baby has the nipple and a big mouthful of breast tissue so that the nipple extends deep into baby’s mouth. This is more likely to be comfortable and lead to a good milk supply.
Bear in mind most healthy babies are able to breastfeed without having to follow step by step instructions. If breastfeeding is comfortable and your baby is getting plenty of milk and growing well, it doesn’t matter what your baby’s latch looks like. As the saying goes: if it ain’t broke don’t fix it.
Latching tips before the feed
Look for early feeding cues
Signs that a baby is getting hungry are known as feeding cues. Early feeding cues include a baby sucking his fist or fingers, and your baby turning his head side-to-side with a wide open mouth as he searches for the breast (called rooting). A late feeding cue would be when your baby cries out loud. Offer the breast when your baby shows early feeding cues; it is much easier to feed a calm baby than one who has to get upset first and scream to get fed.


Get comfortable
When sitting or reclining having your back supported will help to avoid getting back ache. It is important that your baby feels stable, secure and comfortable too. If your baby doesn’t feel secure he might wave his arms about during latching or you might feel like he is “fighting the breast”. He may try to hang on with his lips or clamp down on the breast with his jaw if he doesn’t feel safe; this may cause pain for you and lip blisters for him. See Breastfeeding Positions for Newborns for helpful ways to hold your baby whether sitting, reclining, standing or lying down. Bear in mind breastfeeding pillows can have pros and cons, see Do I Need a Breastfeeding Pillow? for more information.


If a breast is very full or heavy
If your breasts are very full or engorged, this can make it difficult for your baby to attach to the breast. If so, expressing a little breast milk by hand or with a breast pump can soften the breast or try reverse pressure softening—a technique to use your fingers to temporarily move fluid deeper into the breast away from the nipple. If a breast is very large or heavy, the weight of it can tend to pull the nipple from baby’s mouth so that they keep slipping into a shallow latch. It’s Ok to support the breast through a feed if this makes breastfeeding more comfortable—see Breastfeeding With Large Breasts for much more information. For help with engorgement see Engorged Breasts.

Let baby use their hands
Some mothers may feel that their baby’s hands or arms are getting in the way of latching. They may be tempted to move those little hands out of the way or cover them with mittens. However, a baby’s hands help him find, move and shape the breast to help him latch successfully so do not cover or restrict them.1 Finding positions that allow a baby to use his hands constructively and cradle or hug the breast in his arms can be helpful. Babies use all their senses (smell, sight, touch, hearing, taste) to breastfeed. Christina Smillie compares covering hands in mittens with blindfolding a baby (covering their eyes) because it similarly removes one of the senses ie touch.2 See Scratch Mittens and Breastfeeding for more information.

Steps for a comfortable latch
#1 Positioning baby
Hold your baby close to your body in one of the Breastfeeding Positions for Newborns. In reclining positions your baby will already be in a stable position, fully supported against your body. In more upright positions eg cradle hold, cross cradle or rugby hold; make sure your baby is tucked in close and well supported. Check that your baby does not need to turn his head to the side to breastfeed as this makes it very difficult to swallow. You may need to turn your baby onto his side if you are in an upright position so that his tummy is in contact with your tummy/breast and he is not lying on his back with his head turned to one side.


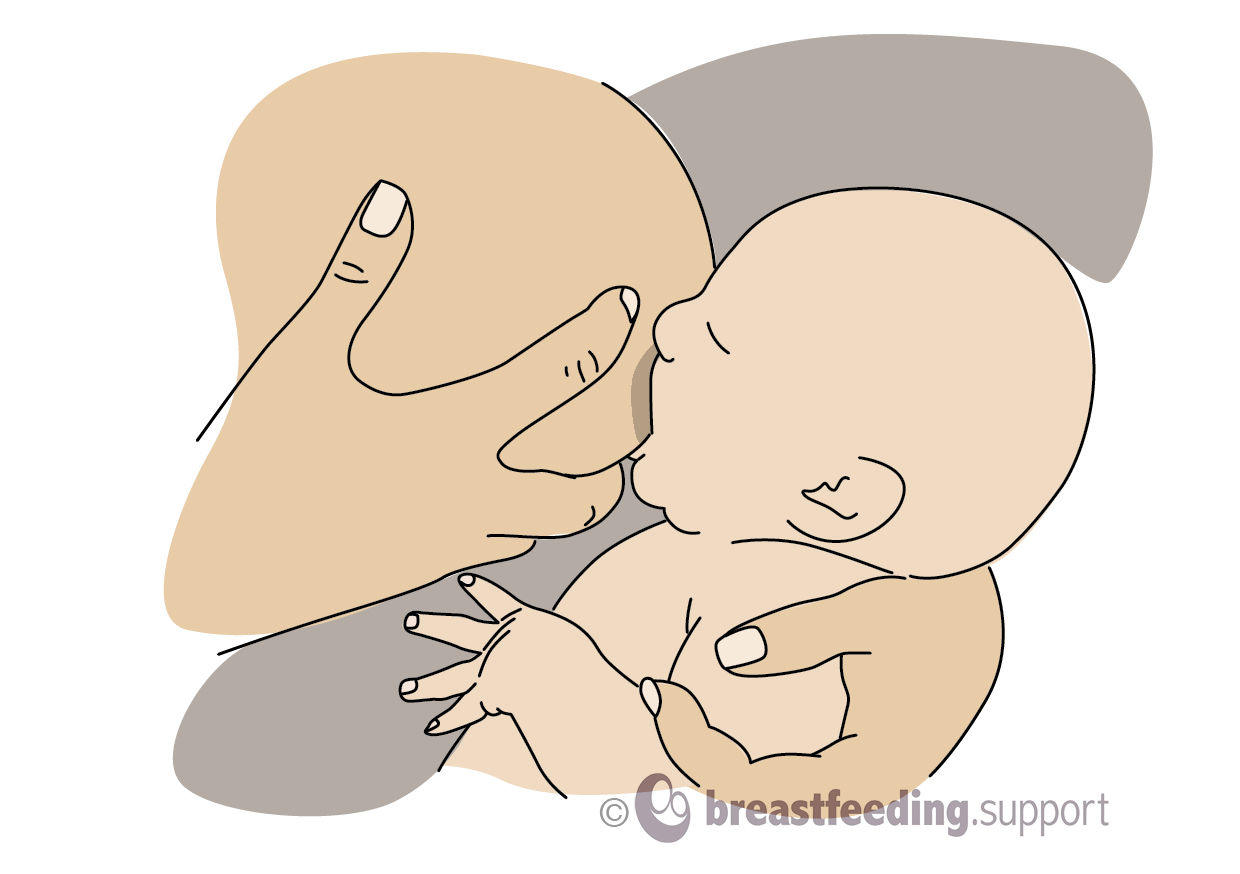
#2 Nose to nipple
In upright positions try holding your baby so that his nose is just level with the nipple (“nose to nipple”) before he opens his mouth to take the breast. This helps your baby to attach with more of the breast beneath the nipple in his mouth than the breast above it (sometimes called an “asymmetric latch”, see #7 below). In reclining positions your baby will have more control to move himself into the right position using his feeding reflexes.

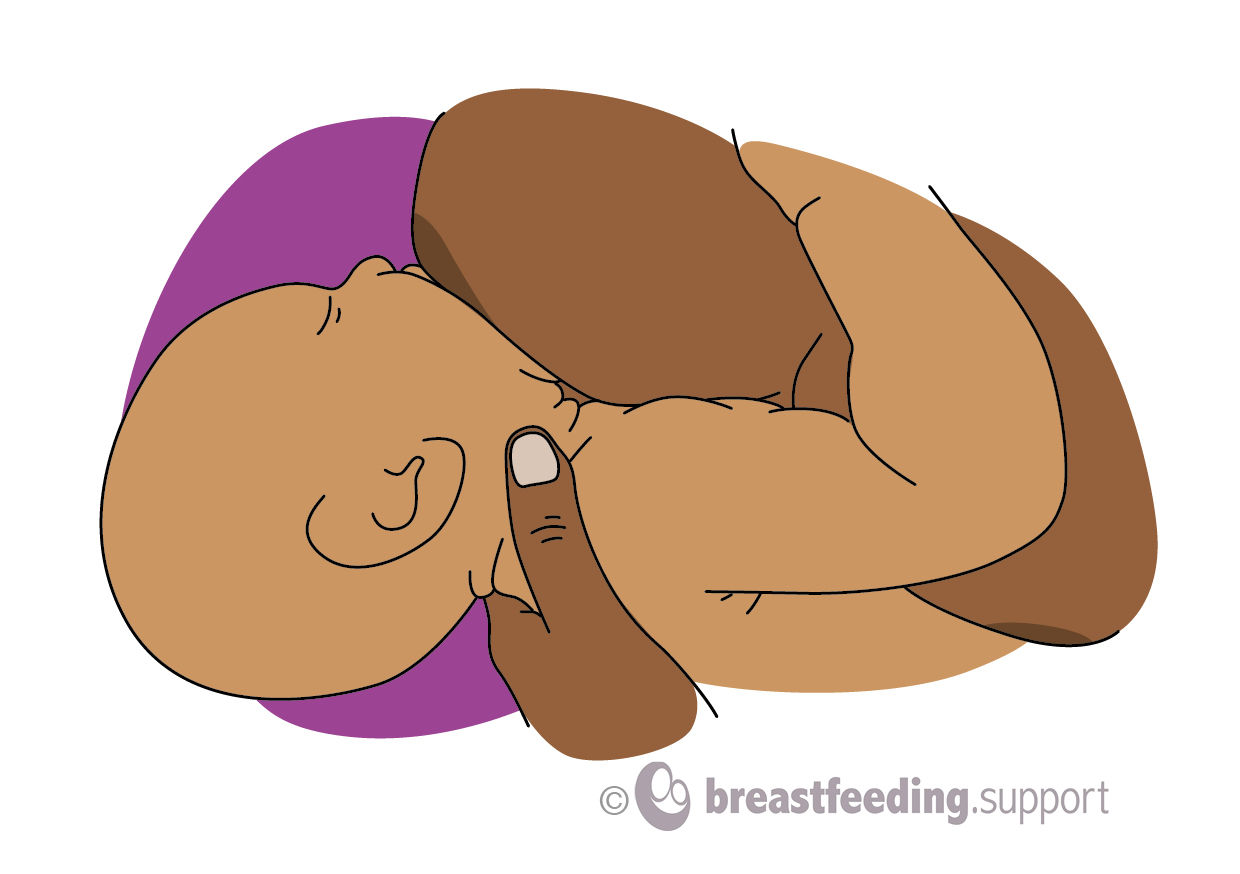
#3 Don’t hold the back of your baby’s head
- A baby needs to be able to tip his head back slightly as he opens his mouth wide to attach to the breast. If your baby can feel your hand holding the back of his head, it may prevent him from tipping his head back and can trigger a reflex to push his head against your hand. This will move him away from the breast instead of towards it.
- Supporting your baby with a hand behind their shoulders rather than with a hand on the back of their head helps your baby to latch more easily. If you feel your baby’s head needs more support, try reclining more so that their weight is fully supported on your body.
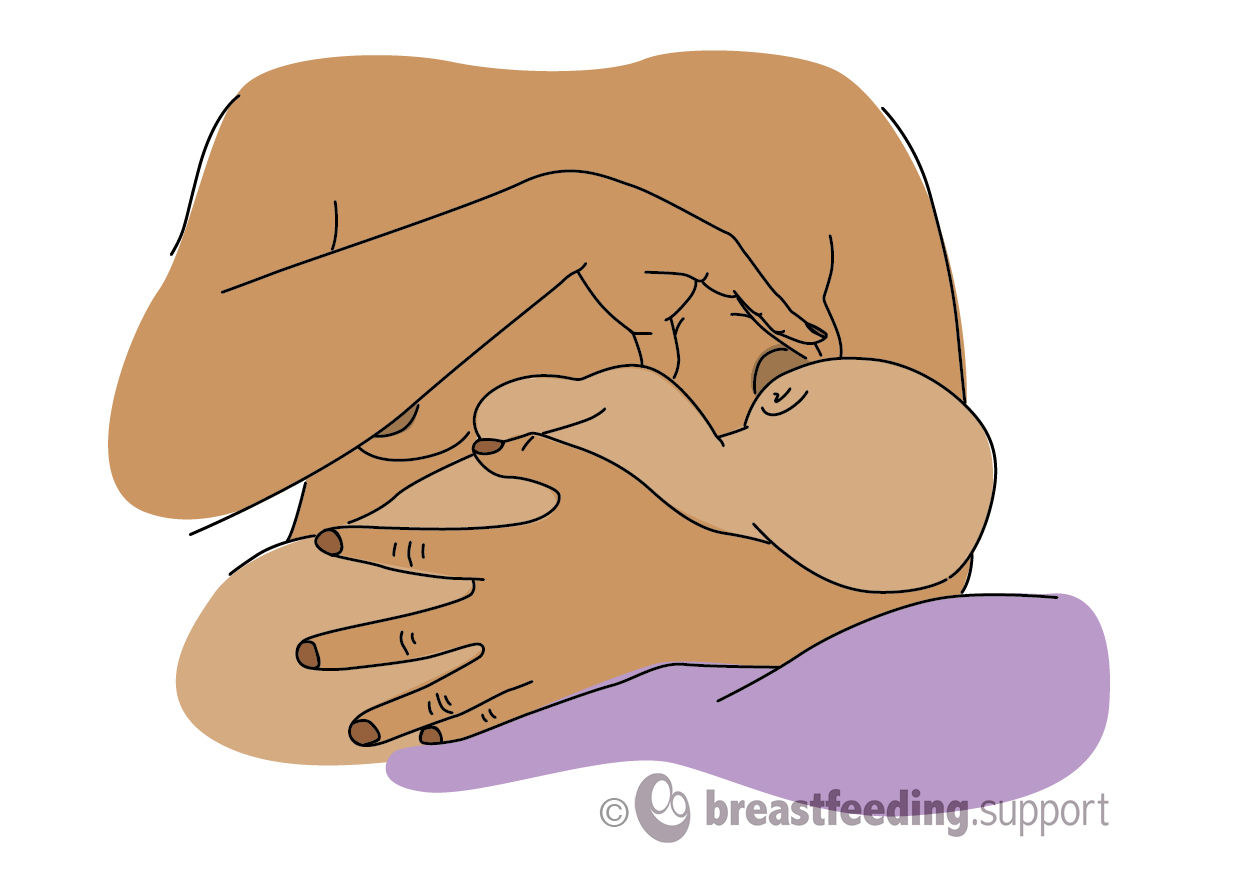
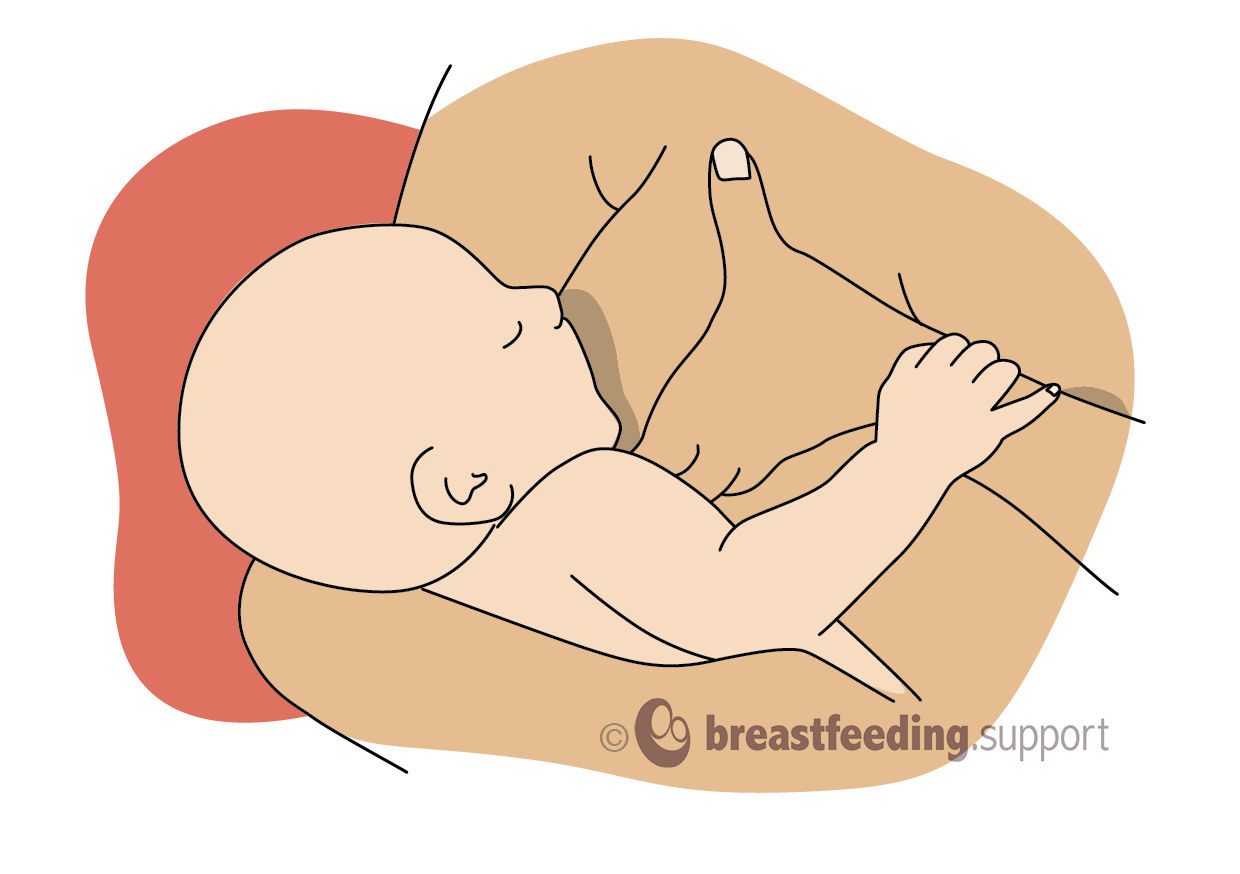
#4 Shaping the breast
- If a baby needs a little extra help to latch deeply, shaping or flattening the breast to fit your baby’s mouth helps some babies to get a bigger mouthful of breast—just as you might flatten a big sandwich full of salad with your fingers before taking a bite. You may hear this called an “assisted latch”.
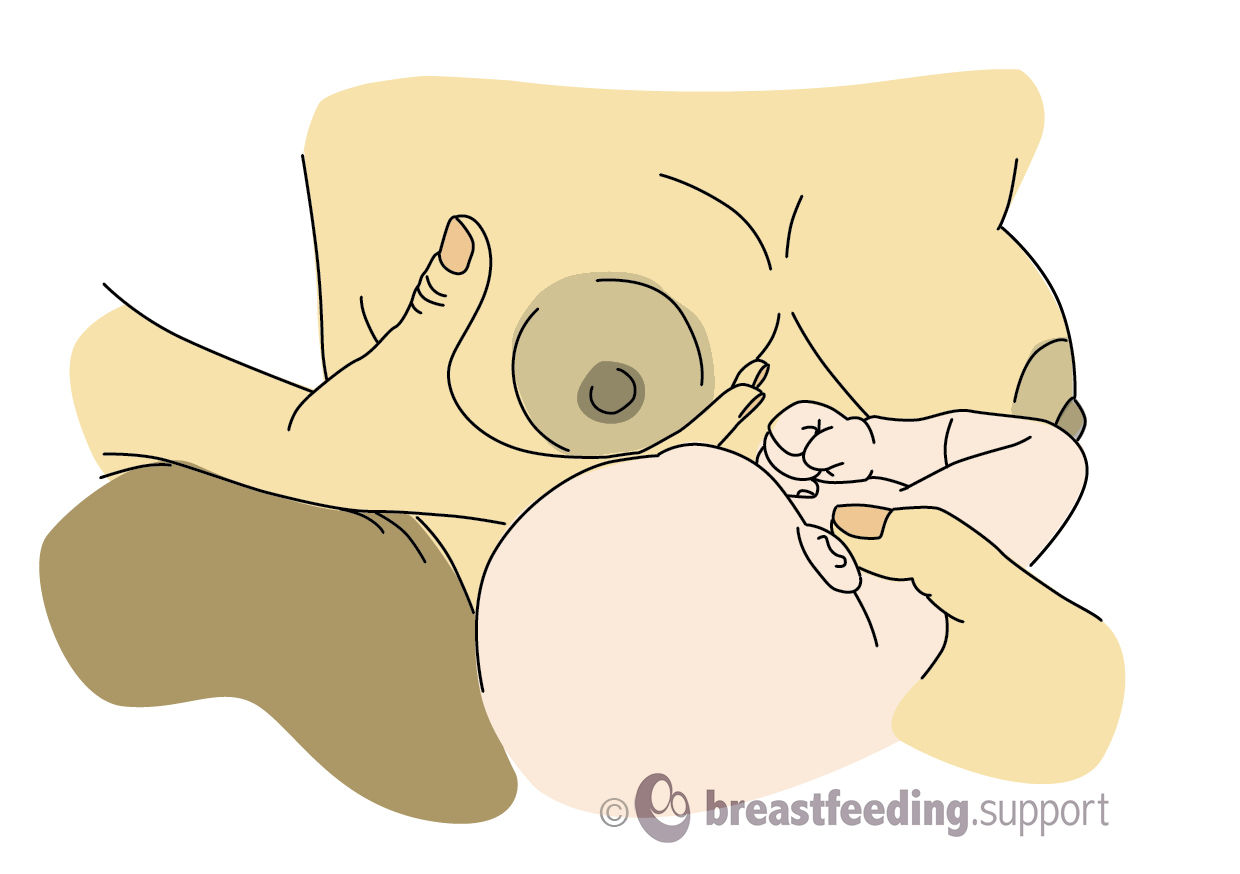
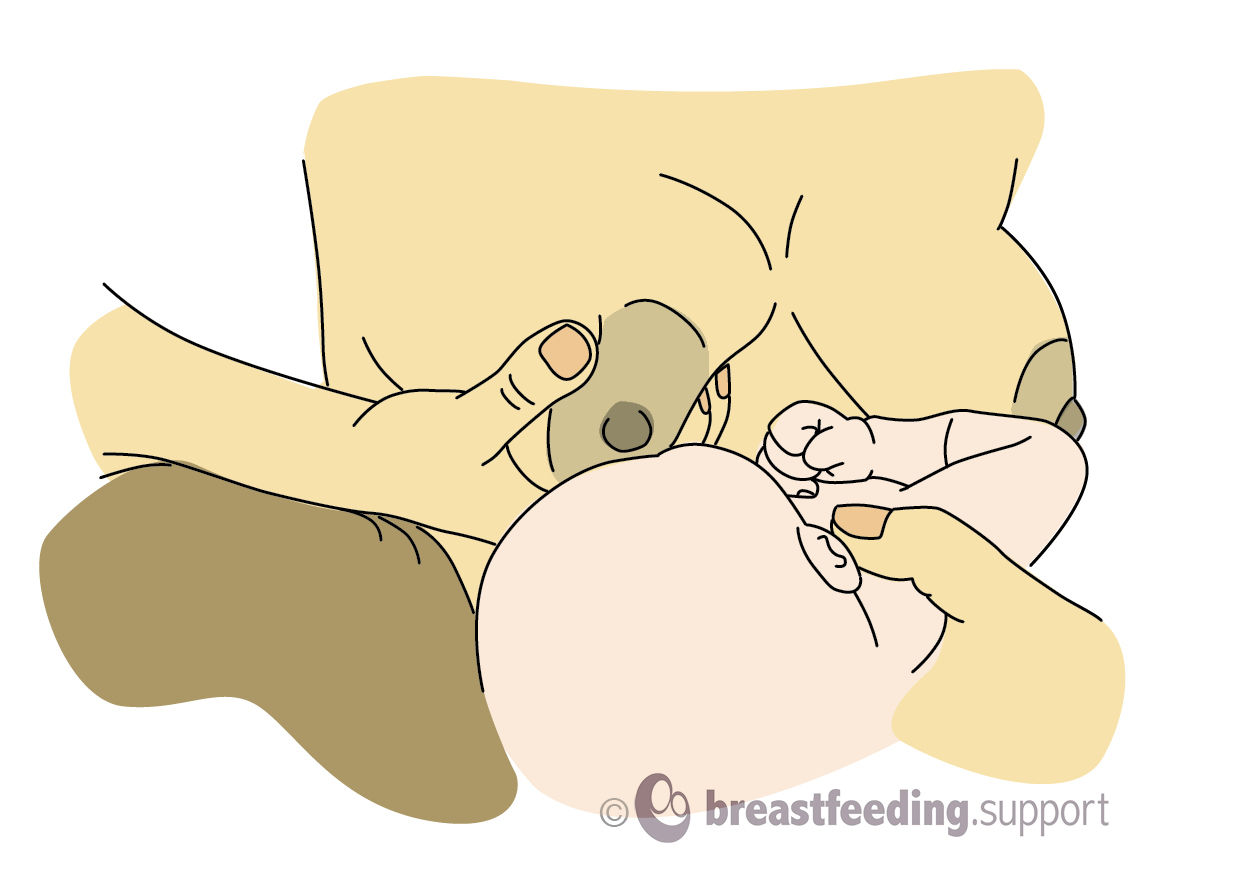
- There are several variations. Some mothers shape the breast by cupping their thumb and fingers around the breast (called a “C” hold or “U” hold), others use two fingers in a “scissor” or “V” hold”. Some mothers point the nipple upwards to expose more areola by pressing a finger or thumb into the top of the breast behind the nipple. You may hear this called an “exaggerated latch”, “flipple” or “nipple flick”.
- Exactly where to place your fingers and compress the breast will depend on the angle your baby is approaching the breast from. Take care not to make it harder for your baby to latch by shaping the breast into a bigger mouthful instead of a smaller one.
- If you do shape or hold the breast, keeping your fingers well away from the nipple will ensure your baby can still get a deep mouthful of breast tissue.
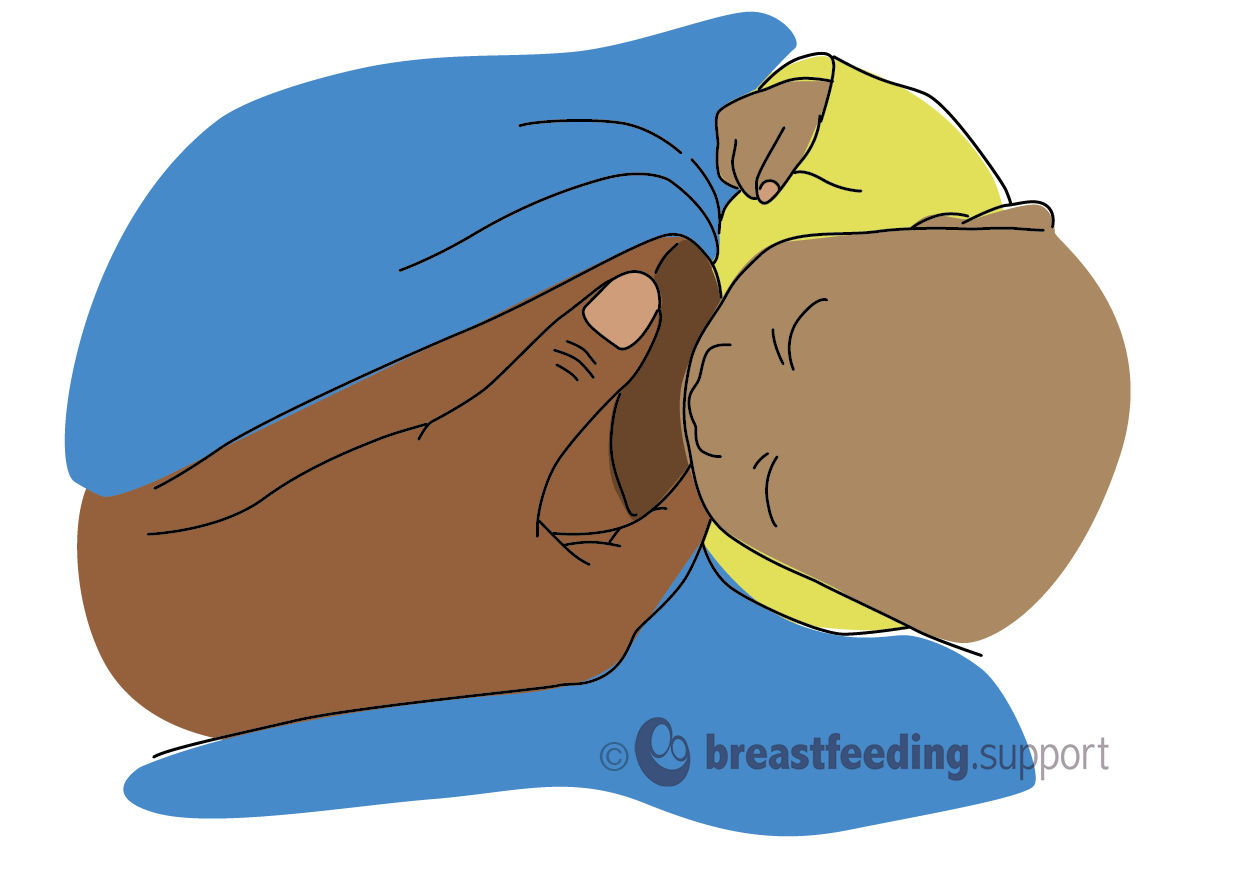
#5 Encourage a wide gape
- A really wide gape as baby latches helps them to get a deeper mouthful of breast tissue as well as the nipple. A reclining position with your baby on his tummy automatically triggers the feeding reflex to search for the nipple with a wide mouth.
- If you are helping your baby to latch in one of the upright positions, make sure your baby can feel your breast against his face so he knows to start searching and opening his mouth (rooting). At the moment when his mouth is widest, bring him closer into the breast towards the underside of the nipple by pulling his shoulders closer towards you (not by pushing the back of his head).
- Remember to bring baby to the breast rather than leaning forward to put your nipple in his mouth as if it was a bottle.
#6 Supporting the breast, optional
Once baby has grasped a big mouthful of breast tissue in an assisted latch the mother can often relax her hand and let go of the breast. Some mothers may prefer to continue to provide some support to the breast during the feed particularly if they have larger breasts, it depends what feels most comfortable.
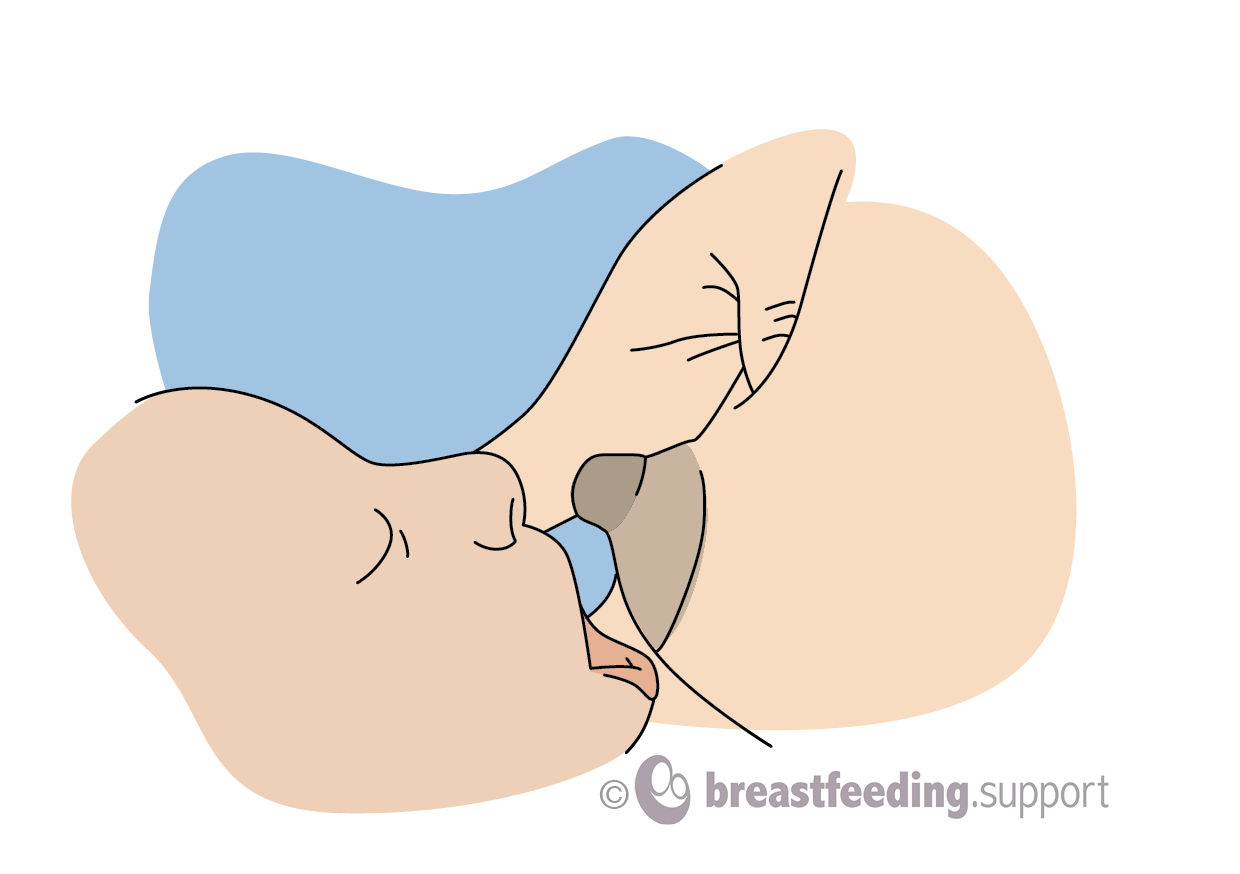
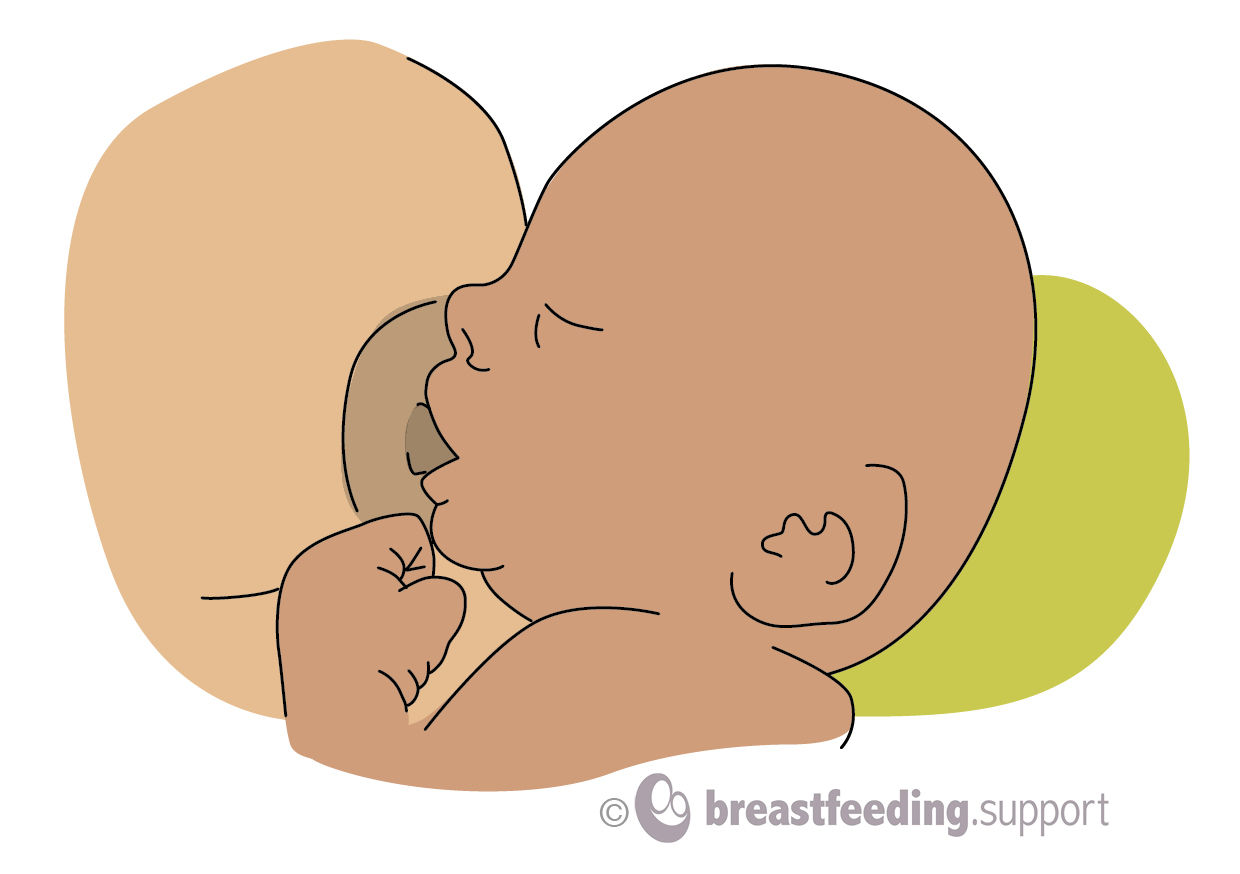
#7 A deep, asymmetric latch
Rather than attaching directly to the nipple, the end goal is for baby to have a big mouthful of breast tissue as well as the nipple in his mouth. The areola is the darker pigmented skin around the nipple. When baby is latched well, you will often be able to see more of the areola above the nipple than you can see below as more of the areola on the underside of the breast will be hidden inside baby’s mouth ie an off-centre or asymmetric latch. In a deep latch baby’s chin and cheeks will often be touching the breast.
Bottom lip turned out
When latched correctly you probably won’t be able to see your baby’s lower lip at all as his chin will be buried in the breast. If breastfeeding is comfortable it doesn’t matter that you can’t see your baby’s lower lip and it is best not to disturb the latch by keep trying to look. However, if breastfeeding isn’t comfortable, you or a helper could gently lift the breast to see what the latch looks like. If the bottom lip is folded in it can often be encouraged out by pressing gently on baby’s chin as he feeds without taking baby off the breast and this may make the latch more comfortable. The top lip rests on the breast, neither turned in nor particularly turned out.




Helping your baby to latch, summary videos
The following video by Global Health Media has a lovely summary of latching tips.
The following is another short clip called The Basics of Latching from Breastfeeding Medicine of Northeast Ohio
Self-latching
In laid-back or reclining positions, babies can often move to the breast and latch quite naturally without your having to worry about “nose to nipple” or “bringing baby to breast”. There are several examples of babies self-latching straight after birth in the following video clip from the Global Health Media Project. Notice how the babies use their hands to help themselves latch. See Why Skin-to-Skin? for further information.
Variations in anatomy
If you have flat or inverted nipples it can sometimes be more difficult for your baby to latch, see Breastfeeding With Inverted Nipples and Flat Nipples for further help. Larger breasted women can find more latching tips in Breastfeeding With Large Breasts.
Summary
Good positioning and attachment (latching) are very important for breastfeeding to run smoothly. Breastfeeding is not supposed to hurt. If after trying these latching tips and reviewing other breastfeeding positions you are still finding breastfeeding painful, see Why Does Breastfeeding Hurt? and contact your breastfeeding specialist for help to find the cause.